
In the two previous installments (one, two) of what has now become my praise of T cells, I explained that the SARS-CoV-2 protein sequences recognized by T cells do not change, likely explaining why vaccines prevent serious disease and death caused by any variant. Today I will explain that virus-specific T cells appear a week after mRNA vaccination when neutralizing antibodies are weakly detectable. Their presence is likely responsible for vaccine-mediated protection against severe disease.
Since the first COVID-19 vaccines were tested in clinical trials, much has been made of their ability to block infection. At ten days after the first vaccine dose, clear protection against severe disease is observed. But at this early time, neutralizing antibodies can barely be detected. That job is likely being done by T cells, the other arm of the adaptive immune response.
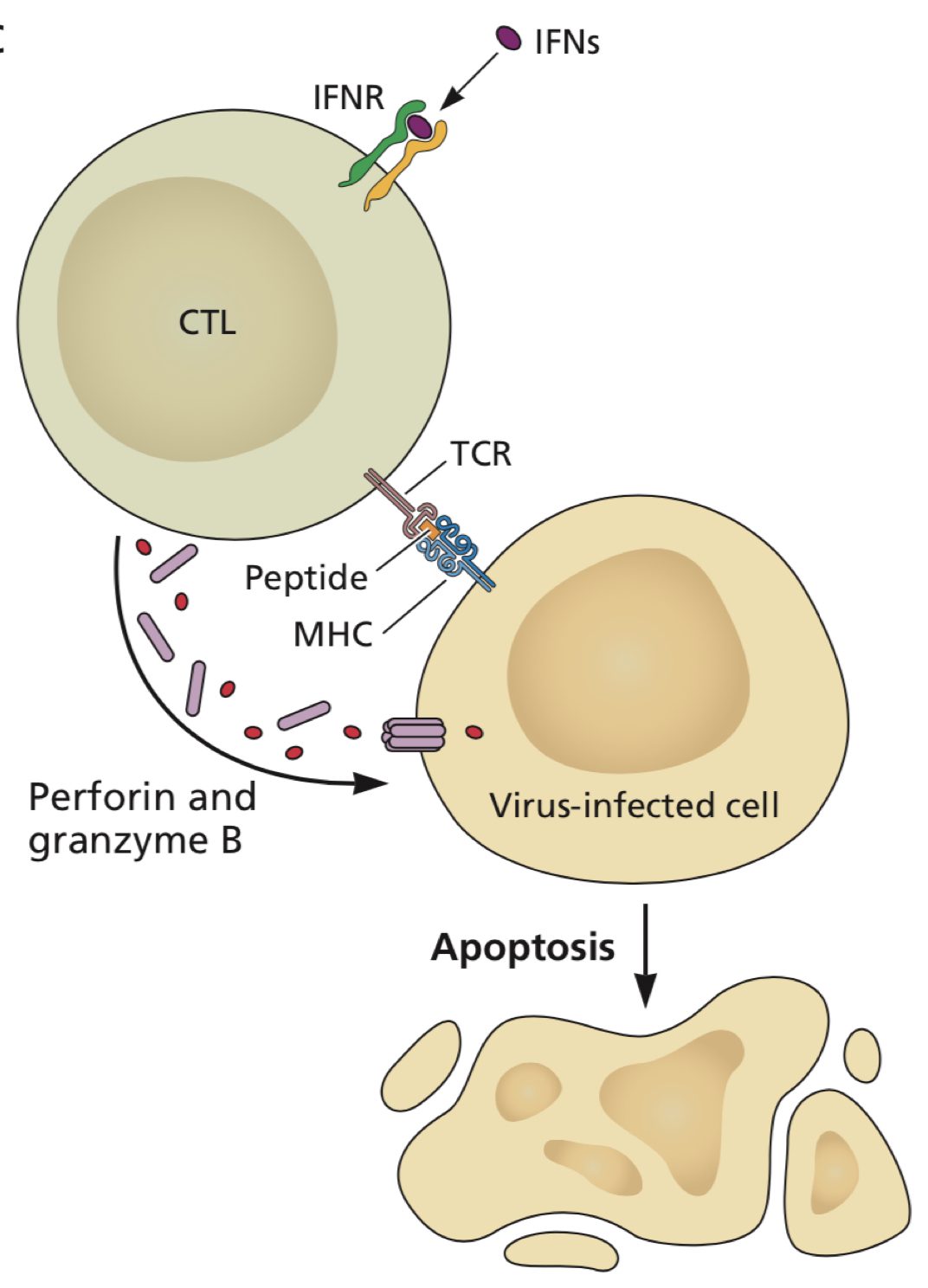
T lymphocytes come in two broad types: CD8+ and CD4+. The former, also known as cytotoxic T lymphocytes (CTLs) can recognize a virus infected cell and kill it (pictured). The latter T cells produce cytokines that are important for maturation of both CTLs and B cells, the antibody-producing cells. The importance of antibody versus T cells in controlling infection depends on the virus. For many viruses, antibody can block infection, but T cells are important for recovery. In COVID-19, antibodies rise late in the course of infection, when virus titers are already declining. This observation is in line with the resolution of infection by T cells.
People with agammaglobulinemia, who cannot make antibodies, or who have been depleted of B cells do not have a serious course of COVID-19, further supporting a role for T cells in preventing severe disease.
During the trials of mRNA vaccines it was observed that protection against severe COVID-19 arose at 10 days after the first inoculation, a time when neutralizing antibodies are barely detectable in serum. The logical candidate for this effect is the T cells.
To address this question, a group of mRNA vaccine recipients were sampled at different times after the first and second doses. CD8+ T cells in blood were examined for the ability to recognize a few spike-specific epitopes. A rapid and substantial induction of CD8+ T cells in these individuals was observed beginning at 6-8 days after the first vaccine dose. At this time, neutralizing antibodies in sera of these subjects were barely detectable. CD8+ T cell numbers are substantially increased by the second vaccine dose, which also leads to much higher levels of neutralizing antibodies. CD4+ T cells are also detected after the first vaccine dose and likely coordinate the expansion of CD8+ T cells and B cells.
mRNA vaccination also induces spike-specific memory B and T cells which circulate for at least several months. Their exact longevity remains to be determined by longer term studies.
The gradual escape of multiple variants of concern from neutralization by sera from vaccinated individuals has been met with alarm by public health officials. At least one prominent leader has suggested that the virus might even mutate so as to escape vaccine protection. An even cursory examination of the facts reveals otherwise. Despite reduced neutralization by vaccine-induced antibodies, vaccine recipients are still protected from severe disease and death by all variants. In contrast to changing B cell epitopes, T cell epitopes do not change in any variant. Furthermore, virus-specific T cells are induced early after the first mRNA vaccine dose, and confer protection against severe COVID-19 at a time when neutralizing antibodies are barely detectable. These observations indicate that T cells will save us from COVID-19.
In vaccinology, the correlate of protection refers to what is needed – antibodies or T cells – to protect from infection or disease. High levels of antibodies appear to correlate with protection against infection by SARS-CoV-2. However, when antibody levels decline, as they always do after infection or vaccination, infection can no longer be prevented. In this case, protection against severe disease and death is accomplished by T cells.
Hi Dear Vincent
Thank you very much for your perfect article..
Right on, as usual Vince. It seems that even though coronaviruses have a gene editing function among their gene products, it isn’t strong enough to prevent the evolution and dissemination of spike protein variants. The delta variant is worse than the ancestral form, and nobody really knows whether further variants of the delta or of other current strains might be worse yet in terms of infectivity and morbidity. This is all possible because the spike protein, located on the surface of the virus, is exposed to the attentions of T- and B-cells and antibodies. For this reason, we should not forget about trying to target viral features that are NOT on the surface, such as the viral RNA polymerase. One can do that simply by taking a scant tsp of CsCl mixed in a glass of juice (to hide the saltiness), waiting ~8hrs, and then eating a banana (to rebalance electrolytes). Repeat 3-4X. Note that CsCl is FDA-approved for clinical use.
Pingback: COVID Tracker: The virus continues its rampage. - Mission Local
HI Vincent, I agree with your conclusions, but this statement is inaccurate:
“T cell epitopes do not change in any variant”.
Delta has at least one mutation that does lead to T cell escape (see “SARS-CoV-2 spike L452R variant evades cellular immunity and increases infectivity”. https://linkinghub.elsevier.com/retrieve/pii/S1931312821002845)
This is an area we are actively working in, and our preprint also shows that the Beta variant has mutations that affect T cell recognition (Loss of recognition of SARS-CoV-2 B.1.351 variant spike epitopes but overall preservation of T cell immunity https://www.medrxiv.org/content/10.1101/2021.06.03.21258307v1). In the next version of the paper we identify 3 mutations in Beta that lead to this loss of response. However, we found that this affects only a small portion of the T cell response (15%), so 85% of the response is preserved.
Because T cells target many epitopes across Spike (and many other viral proteins, but of course the Spike ones are important since that’s the vaccine antigen), and we all have different genetic HLA backgrounds, so its our immune diversity that will be what preserves the T cell response to all SARS-CoV-2 variants, even if some of the epitopes are affected.
Thanks for this hopeful article.
Thanks for the article. Ampligen could be the answer. Ampligen activates the TLR3 pathway and promoted an accumulation of killer t-cells. I’ll be watching their Phase 2a human challenge trial closely as an intranasal antiviral prophylactic therapy.
I have gotten several direct reports of young people in California who were fully vaccinated with Pfizer or Moderna that got a severe enough case of Delta variant to require hospitalization with oxygen. Of the 2 I was able to get history for, both were early 20’s, and smoked non-tobacco products. They used flavor-vapes and they smoked high (30%+) THC marijuana regularly. They also did dabs, which are a THC concentrate.
Pingback: T cells will save us from COVID-19, part 3 - Virology Hub
Professor,
Could you respond to this video? https://youtu.be/5a7PLv9JkF4
It states that areas where Pfizer and Moderna conducted their trials with participants living in the same area where variants were introduced. The focal assumption is that the numerous variety in covid vaccines are all leaky, leading to immunity escape, which breeds more virulent strains of coronavirus.
This assumption on an imperfect vaccine is not new. Similarly, the virulent marek’s vaccine also caused a commotion. To which, I read your response to the similar standpoint dated in 2015. However, it still puzzles me as to why the variants coincided with the geographic in which clinical trials volunteers inhabited?
I’m super confused on this issue. Please address this! Thank you
I will attempt to answer Theresa’s question to Prof. Racaniello. I watched the video. It was such a hodgepodge of side- and central issues to the COVID-19 pandemic that you can’t help but be confused. From choosing a supplier because there are not enough bodybags (a side issue) to viruses throwing off variants ( a central issue) to perfection (or not) of vaccines (a twist on a different central issue), the starting place is the fact that RNA viruses are not a single entity. Each viral genome differs from its friends and neighbors at one or more positions ALL THE TIME. Every variant is already present in each patient’s viral load. The predominant variant has evolved – it has been selected for maximum efficiency by its interactions with both host and other viral features. There are 30,000 nucleotides in a coronavirus genome. There are at least 10e12 viruses in each patient. The numbers are staggering. It is very Darwinian, and the Darwin controversy is still with us since the 1860’s. As for the perfection of vaccines, each vaccine is perfect unto itself, but it’s self is not Darwinian – it doesn’t change according to its efficiency, so with time the virus will evolve away from the vaccine. Modern RNA technology permits the vaccine maker to quickly alter the vaccine to suit the most recent viral variant – but eventually the virus will again evolve away from the vaccine. As Watson and Crick put it: ‘biology is leaky’. As Tucker Carlson put it: “If you don’t think this is a conspiracy, then you don’t know New York.” And if this doesn’t answer your question, then you will have to turn back to Prof. Racaniello.